Introduction
Background
Rheumatoid arthritis (RA) is a systemic autoimmune inflammatory disease characterized by synovitis and serositis (inflammation of the lining surfaces of the joints, pericardium, and pleura), rheumatoid nodules, and vasculitis. The hallmark feature of the disease is persistent symmetric polyarthritis (synovitis) that affects the hands and feet, although any joint lined by a synovial membrane may be involved. In addition to articular deterioration, systemic involvement may lead to weight loss, low-grade fever, and malaise. The severity of RA may fluctuate over time, but chronic RA most commonly results in the progressive development of various degrees of joint destruction, deformity, and a significant decline in functional status.
Juvenile rheumatoid arthritis (JRA; demonstrated in the images below) is the most common form of childhood arthritis. The cause remains unknown. For most patients, the immunogenic associations, clinical pattern, and functional outcome are different from adult onset RA.
Ankylosis in the cervical spine at several levels due to long-standing juvenile rheumatoid arthritis (also known as juvenile idiopathic arthritis).

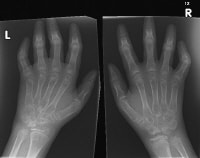
Widespread osteopenia, carpal crowding (due to cartilage loss), and several erosions affecting the carpal bones and metacarpal heads in particular in a child with advanced juvenile rheumatoid arthritis (also known as juvenile idiopathic arthritis).
The diagnostic criteria for JRA are onset occurring when younger than 16 years, persistent arthritis in 1 or more joints for at least 6 weeks, and exclusion of other types of childhood arthritis. The key points that characterize the diagnosis of JRA are as follows:
- Arthritis must be present. Arthritis is defined as the presence of swelling, the presence of effusion, or the presence of 2 or more of the following signs: limited range of motion (ROM), tenderness, pain on motion, or joint warmth.
- Arthritis must persist for at least 6 weeks.
- Other causes of chronic arthritis in children must be ruled out.
- No specific laboratory or other test can establish the diagnosis of JRA.
Recent studies
In a study of 39 women with either RA or osteoarthritis of the lower limb, Williams et al investigated whether, in older women with these conditions, balance and gait stability could be improved via an individualized home program of balance-training exercise. The patients (mean age 69.3 years) underwent a 4-month program of balance exercises conducted by a physical therapist. Prior to exercise training, 64% of patients reported having fallen during the previous 12 months, and 42% of patients had a moderate fall-risk score. Following the 4-month program, the patients demonstrated improvement on most balance measurements, including their fall-risk score and measurements of activity level, fear of falling, functional reach, and step width. Improvements were also seen in patients' body mass index and in their sit-to-stand rising index.1
In a study of 39 women with either RA or osteoarthritis of the lower limb, Williams et al investigated whether, in older women with these conditions, balance and gait stability could be improved via an individualized home program of balance-training exercise. The patients (mean age 69.3 years) underwent a 4-month program of balance exercises conducted by a physical therapist. Prior to exercise training, 64% of patients reported having fallen during the previous 12 months, and 42% of patients had a moderate fall-risk score. Following the 4-month program, the patients demonstrated improvement on most balance measurements, including their fall-risk score and measurements of activity level, fear of falling, functional reach, and step width. Improvements were also seen in patients' body mass index and in their sit-to-stand rising index.1
Pathophysiology
The diagnosis of rheumatoid arthritis (RA) must be considered in any patient with polyarticular inflammatory arthritis, especially if both the hands and feet are involved. The early phase of the disease is characterized by the following features:
- Joint swelling that may affect joint margins
- Joint tenderness upon palpation
- Systemic malaise
- Loss of energy
- Severe morning stiffness that limits function and generally lasts more than an hour
A classic feature of the illness is the symmetry of involvement. If synovial-based inflammation persists over time, permanent damage to tendons, ligaments, and cartilage occurs, as does subchondral bone destruction, with resultant joint deformity and limited motion. Inflammation and deformity are nearly always seen in the hands and feet (see the images below). However, involvement of the knees, hips, and shoulders accounts for significant morbidity that leads to work disability in a large percentage of patients.2
Rheumatoid changes in the hand. Photograph by David Effron MD, FACEP.

Prominent juxta-articular osteopenia in all interphalangeal joints in a patient with rheumatoid arthritis of the hands.

A major difference in the pathophysiology of RA versus osteoarthritis or mechanical joint problems is the presence of extensive synovial inflammation. The characteristic signs of inflammation were stated by Celsus as "rubor et tumor cum calore et dolore," meaning redness and swelling with heat and pain. Galen later added "et functio laesa" (disturbed function) to the characteristic signs of inflammation. Joint tenderness, swelling, stiffness, and pain on motion are the features of inflammation experienced by patients with RA.
Frequency
United States
The prevalence rate of rheumatoid arthritis is approximately 1% of the population (range 0.3-2.1%).
Race
Rheumatoid arthritis is observed throughout the world and affects persons of all races.
Sex
Women are affected by rheumatoid arthritis (RA) approximately 3 times more often than men.3 Sex differences diminish in older age groups.4
A study from Denmark investigated whether the higher rate of RA among women could be linked to certain reproductive risk factors.5 Reviewing the cases of men and women who had been hospitalized with RA between 1977 and 2004, the authors found that the rate of RA was higher in women who had given birth to just 1 child than it was in women who had delivered 2 or 3 offspring. (However, no increased rate was found in women who were nulliparous or who had a history of lost pregnancies.)
The study also found a higher RA risk among women with a history of preeclampsia, hyperemesis during pregnancy, or gestational hypertension. The authors suggested that this portion of the data indicated that a reduced immune adaptability to pregnancy may exist in women who have a predisposition to the development of RA or that there may be a link between fetal microchimerism (in which fetal cells are present in the maternal circulation) and RA.
A study from Denmark investigated whether the higher rate of RA among women could be linked to certain reproductive risk factors.5 Reviewing the cases of men and women who had been hospitalized with RA between 1977 and 2004, the authors found that the rate of RA was higher in women who had given birth to just 1 child than it was in women who had delivered 2 or 3 offspring. (However, no increased rate was found in women who were nulliparous or who had a history of lost pregnancies.)
The study also found a higher RA risk among women with a history of preeclampsia, hyperemesis during pregnancy, or gestational hypertension. The authors suggested that this portion of the data indicated that a reduced immune adaptability to pregnancy may exist in women who have a predisposition to the development of RA or that there may be a link between fetal microchimerism (in which fetal cells are present in the maternal circulation) and RA.
Age
Although rheumatoid arthritis (RA) can occur at any age, the incidence increases with advancing age. The peak incidence of RA occurs in individuals aged 40-60 years.
Clinical
History
Stiffness of the joints is a major symptom in any type of arthritis and particularly in rheumatoid arthritis (RA). Frequently, RA is accompanied by "morning stiffness." Other inflammatory conditions, such as polymyalgia rheumatica and ankylosing spondylitis, also may be accompanied by morning stiffness. The severity of stiffness may better differentiate a primary inflammatory process from other joint processes. Edema of the synovium and periarticular structures contributes to stiffness in RA by mechanically interfering with the usual biomechanics of the joint. With normal sleep patterns, stiffness is most pronounced in the morning, in part due to redistribution of interstitial fluid while sleeping.
Pain is a significant problem for most patients with RA. Although the assessment is subjective, the patient's relief from pain is the objective for treatment. Swollen joints with an applied load or joints with rapidly evolving effusions may be extremely painful due to high intra-articular pressures that lead to excessive stresses on the extensively innervated periarticular supporting structures.
Physical
Effects of rheumatoid arthritis on particular joints
Fingers
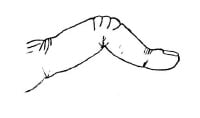
The boutonniere deformity, demonstrated in the image below, describes nonreducible flexion at the proximal interphalangeal (PIP) joint along with hyperextension of the distal interphalangeal (DIP) joint of the finger. This deformity occurs as a result of synovitis stretching or rupturing of the PIP joint through the central extensor tendon with concomitant volar displacement of the lateral bands. When the lateral bands have subluxed far enough to pass the transverse axis of the joint, they become flexors of the PIP joint. Hyperextension of the DIP joint occurs as the tendons shorten with time. A compensatory and reducible hyperextension may occur at the metacarpophalangeal (MCP) joint. Consequences of boutonniere deformity are loss of thumb mobility and pincher grasp.
Boutonniere deformity.
Swan-neck deformity of the finger describes hyperextension at the PIP joint with flexion of the DIP joint. The deformity may be initiated by (1) disruption of the extensor tendon at the DIP joint with secondary shortening of the central extensor tendon and hyperextension of the PIP joint or (2) volar herniation of the PIP joint capsule due to weakening from chronic synovitis with subsequent tightening of the lateral bands and central extensor tendon. The lateral bands may become shortened over time and lie dorsally, limiting PIP flexion and ineffectively extending the DIP joint.
Tightness of intrinsic muscles (eg, interossei, lumbricals) may cause major declines in mobility of the fingers. This characteristic is ascertained on examination when the PIP joint cannot be flexed while the MCP joint is fully extended but can be flexed if the MCP is in flexion (Bunnell test); primary PIP joint pathology would be evident with the MCP joint in either position. To assess this accurately, the phalanx must be aligned with the metacarpal since the intrinsics on the ulnar side are slack when ulnar deviation at the MCP joint exists, thus allowing more motion.
Flexor tenosynovitis of the fingers is common and suggests a poor prognosis. Tenosynovitis is defined as inflammation of the tendon and its enveloping tendon sheath. "Triggering" of the finger occurs when thickening or nodule formation of the tendon interacts with the concomitant tenosynovial proliferation, trapping the tendon in a flexed position (stenosing tenosynovitis). Tendon rupture may occur due to infiltrative synovitis in the digit or bony erosion of the tendon at the wrist (especially the flexor pollicis longus).
Arthritis mutilans (ie, opera glass hands) results if destruction is severe and extensive, with dissolution of bone. In the small joints of the hands, the phalanges may shorten and the joints may become grossly unstable. Pulling on the fingers during examination may lengthen the digit much like opening opera glasses, or the joint may bend in unusual directions merely under the pull of gravity.
Metacarpophalangeal joints
Seen in the image below, 2 typical deformities that alter the alignment of the palmar skeletal arches and the stability of the fingers may occur at the MCP joints: volar subluxation and ulnar deviation. Most cases of ulnar deviation are accompanied by counterpoised radial deviation of the wrist, roughly proportional to the degree of ulnar deviation of the fingers. The volar plate is firmer and more substantial than other portions of the MCP joint capsule and, therefore, effectively limits extension and dorsal movement at the joint. The greater relative strength of the flexor muscles as compared with the extensor muscles causes volar migration of the proximal phalanx after synovial-based inflammation has weakened ligament and tendon insertions about the MCP joint capsule.
Subluxation in the metacarpophalangeal joints, with ulnar deviation, in a patient with rheumatoid arthritis of the hands.

Ulnar deviation occurs after synovitis has led to stretching and attenuation of the volar plate and collateral ligaments, allowing dislocation of the flexor tendon volarward and ulnarward. The supporting structures of the extensor tendons also may become attenuated or destroyed by synovial distension and invasion, loosening the tendons so that they no longer ride centrally and dorsally over the metacarpal head but move into the cleft between the MCP joints. If the extensor tendon subluxation is beyond the transverse axis of the MCP joint, the tendon becomes a flexor at that joint, further limiting the active extension of the fingers.
Wrists
Multiple deformities may occur in the wrist. Disruption of the radioulnar joint with dorsal subluxation of the ulna (caput ulna), as well as rotation of the carpus on the distal radius with an ulnarly translocated lunate, is common. The combination of an ulnar drift of the fingers and carpal rotation is known as a zigzag deformity. Shortening of the carpal height (noted on radiographs), due in part to cartilage loss, is seen with rotational deformities.
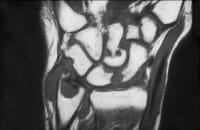
Dorsal subluxation of the ulna often allows the ulnar styloid to be depressed volarly on examination, much like depressing a piano key. Subluxation may lead to rupture of the extensor tendons of the little, ring, and long fingers, because the end of the distal ulna is roughened secondary to erosion of bone and may abrade the tendons as they move back and forth during normal hand function, much like a rope being frayed while rubbing over a sharp rock. This process is especially likely to lead to tendon rupture if there is associated tenosynovitis. (See the image below.)
Coronal, T1-weighted magnetic resonance imaging (MRI) scan shows characteristic pannus and erosive changes in the wrist in a patient with active rheumatoid arthritis. Courtesy of J. Tehranzadeh, MD, University of California at Irvine.
Entrapment neuropathy may result from synovitis about the flexor tendons. Entrapment of the median nerve as it passes through the carpal tunnel leads to decreased sensation on the palmar aspect of the thumb, index finger, and long finger and on the radial aspect of the ring finger; weakness and atrophy of the muscles in the thenar eminence also occurs. The less frequent entrapment of the ulnar nerve at the wrist causes decreased sensation over the little finger and the ulnar aspect of the ring finger and decreased interosseous muscle strength and mass.
Elbow
Elbow involvement often is detected by palpable synovial proliferation at the radiohumeral joint and commonly is accompanied by a flexion deformity, such as in contractures. Olecranon bursal involvement is common, as are rheumatoid nodules in the bursa and along the extensor surface of the ulna. Nodules are clearly seen in the image below.
Rheumatoid nodules at the elbow. Photograph by David Effron MD, FACEP

Shoulders
Rheumatoid arthritis (RA) commonly involves the shoulders. RA in the shoulders is manifested by tenderness, nocturnal pain, and limited motion. Initially, swelling occurs anteriorly, but it may be difficult to detect and is present on examination in a minority of patients at any point in time. Rotator cuff degeneration secondary to synovitis may limit abduction and rotation. Superolateral migration of the humerus occurs with complete tears. Glenohumeral damage leads to pain with motion and at rest and typically leads to severely restricted motion or "frozen shoulder syndrome." Acromioclavicular arthritis is not as frequent or as disabling.
Feet and ankles
The ankle joint itself is rarely involved without midfoot or metatarsophalangeal (MTP) involvement. The ankle does not often deform, as it is a mortise joint. Major structural changes occur in the midfoot and foot due to the combination of chronic synovitis and weight bearing. Posterior tibialis tendon involvement or rupture may lead to subtalar subluxation, which results in eversion and migration of the talus laterally. Midfoot disease leads to loss of normal arch contour with flattening of the feet.
The MTP joints are inflamed in most patients and, due to the heavy loads they bear, commonly become deformed over time. The great toe typically develops hallux valgus (a bunion); subluxation of the phalanx at the MTP joint of the other toes predominantly occurs dorsally. The toes may exhibit compensatory flexion due to a fixed length of the flexor tendons, thus resulting in "hammer toes" (thought to look like piano hammers). The second and third metatarsal heads commonly protrude and may become the primary weight-bearing surface at the MTP joints. Calluses and pain upon weight bearing result.
Knees
Knees may develop large effusions and abundant accumulation of synovium. Knee effusions and synovial thickening are common and are easily detected during the early course of the disease. Persistent effusions may lead to inhibition of quadriceps function by spinal reflexes, resulting in subsequent atrophy. Instability may develop after progressive loss of cartilage and weakening of ligaments; deformity may include genu valgus or varus and flexion deformities. The energy expenditure to stand or walk significantly increases if there are flexion deformities of the knees.
Hips
The hip is commonly involved in RA; however, because of its deep location, its involvement is not always readily apparent early on during the course of the disease. Hips are difficult to examine by direct inspection or palpation. Limited motion or pain on motion and weight bearing are the hallmarks of hip involvement. The Patrick maneuver (flexion, external rotation, and abduction) is abnormal in this situation. A flexion deformity may be demonstrable by conducting a Thomas test. The Thomas test is performed by flexing one hip (with the patient supine) while restricting pelvic motion by keeping the other hip in the neutral position on the examination table. If the hip cannot be maintained in the neutral position, a contracture is present.
Cervical spine
Neck pain on motion and occipital headache are common manifestations of cervical spine involvement (seen in the image below). Most patients with cervical spine involvement have a history of the disease for more than 10 years. Clinical manifestations of early cervical spine disease consist primarily of neck stiffness that is perceived throughout the entire arc of motion. The atlantoaxial joint is a synovial-lined joint and is susceptible to the same proliferative synovitis and subsequent instability seen in the peripheral joints. Patients with severe destruction in the hands (arthritis mutilans) are very likely to have symptomatic cervical spine abnormalities, as are those patients taking significant amounts of corticosteroids for control of RA.
Lateral view of the cervical spine in a patient with rheumatoid arthritis shows erosion of the odontoid process.

Neurologic involvement ranges from radicular pain to a variety of spinal cord lesions that may result in weakness (including quadriparesis), sphincter dysfunction, sensory deficits, and pathologic reflexes. Transient ischemic attacks and cerebellar signs may reflect vertebral artery impingement from cervical subluxation or basilar artery impingement from upward migration of the dens. Tenosynovitis of the transverse ligament of C1 may lead to C1-C2 instability. Myelopathy secondary to rupture of the transverse ligament may lead to neurologic deficits. Radiculopathy is most common at the C2 root, although symptomatic subluxations may occur at any level.
Symptoms of cervical myelopathy are gradual in onset and are often unrelated to either the development of or accentuation in neck pain. When neck pain does occur, it frequently radiates over the occiput region in the distribution of the C1-3 nerve roots. The Lhermitte sign, in which tingling paresthesia that descends through the thoracolumbar spine occurs as the cervical spine is flexed, is typically observed.
During the physical examination, it is important to assess the following signs and symptoms4 :
- Stiffness
- On physical examination, stiffness is determined by limitation of motion, which may vary with the time of day. Stiffness due to articular surface derangement or soft-tissue contractures about the joint does not vary with the time of day.
- Severe stiffness in the hands may improve with heat, but it is most effectively relieved with active exercise. These modalities reduce stiffness immediately after application, but unfortunately, they do not prevent the return of stiffness.
- Tenderness
- Direct palpation can elicit joint tenderness.
- Tenderness can vary significantly among patients and with the method of application of force used to elicit tenderness. The examiner should try to apply approximately the same pressure for each patient examined to minimize variation over time.
- The enlarged synovial membrane, periarticular ligaments, and supporting structures are the major pain-sensitive structures.
- Muscles also may become tender, but rarely is this due to myositis. Muscle tenderness is not specific for RA. Severe muscle tenderness should suggest other differential diagnoses including fibromyalgia or a regional pain disorder.
- Bony prominences are generally tender, as periarticular structures tend to be more vulnerable to palpation at these sites.
- Pain on motion
- Pain on motion often is used as a surrogate for tenderness in joints that are difficult to directly palpate due to overlying muscle and other tissues. The areas that are difficult to palpate include the cervical spine, shoulder, and hip.
- Pain on motion of the joint may be due to noninflammatory processes that also interfere with the joint's normal, almost frictionless motion, including damage of cartilage and bone.
- Additionally, joint instability or subluxation causes pain on motion because of musculotendinous imbalances across the joint. Documenting the positions of motion at which pain occurs can be useful.
- Swelling
- Early in the disease process, there is an influx of inflammatory cells into the synovial membrane, with subsequent angiogenesis, proliferation of chronic inflammatory (mononuclear) cells and resident synovial cells, and marked histologic changes—a 2 – cell-layer lining membrane changes to a thickened membrane that often has villous projections into the joint space.
- Enlargement of the synovial membrane is noted on physical examination as thickening of the synovium that may obscure joint margins. This thickening is most evident in the small joints of the hands and feet. In the MCP and MTP joints, the outline of the base of the proximal phalanx may become indistinct, and in the PIP joints of the fingers, a fusiform swelling is noted due to the anatomy of the synovial reflections. (See the image below.)
Soft-tissue swelling and early erosions in the proximal interphalangeal joints in a patient with rheumatoid arthritis of the hands.

- If synovial proliferation is abundant, a doughy texture may be felt due to the resultant soft-tissue mass. Such synovial proliferation is commonly identified in the PIP, MCP, elbow, ankle, MTP, and knee joints, as well as in the flexor tendons of the fingers, the common extensor compartment of the dorsal wrist, and the extensor carpi ulnaris tendon sheath.
- Joint effusions also may contribute to swelling by distending the joint. When the effusion is put under increased pressure with joint flexion, the synovium may be forced between articular structures and a portion becomes trapped and separated from the rest of the joint, forming a Baker cyst. More fluid is forced into the structure with subsequent loading of the distended joint, and a 1-way valve effect may prevent the fluid from returning to the joint.
- Baker cysts, one of which is seen in the image below, may be seen in most peripheral joints and are most commonly recognized in the knee. The larger the effusion, the more likely a painful cyst will develop. Rupture of a Baker cyst at the knee may resemble acute thrombophlebitis with distal dissection of inflammatory joint contents along fascial planes as far as the ankle and dorsal foot.
Anteroposterior radiograph of the knee shows uniform joint-space loss in the medial and lateral knee compartments without osteophytosis. A Baker cyst is seen medially (arrowhead).

- Deformity
- Deformity of the joint may develop over time as articular and supporting structures are damaged by the inflammatory process.
- By the time deformity has developed, the diagnosis of RA is in little doubt; however, recognition of the inflammatory aspects of the arthritis before the development of deformity is required for optimal management of RA. Loss of cartilage from proteolytic and mechanical degradation, combined with stretching and weakening of the periarticular ligaments and their attachments, allows forces acting across the joints to deform them. The small joints in the hands and feet are most commonly deformed in this manner; greater than 10% of patients with RA develop deformity of the small joints of the hands within the first 2 years of the disease, and at least one third develop such deformities over time. Joint instability is seen if disruption of supporting structures has occurred.
- Limitation of motion
- Limitation of motion occurs as a result of articular surface damage, joint and tendon sheath swelling, or alteration of joint supporting structures.
- Effusion may limit joint motion through pain or by causing sufficient tightness of the joint capsule to impede joint mobility.
- Fibrosis involving tendons and muscles may limit normal joint motion and result in flexion contractures.
- Joint deformities and subluxations invariably limit motion because of mechanical factors.
- Extra-articular manifestations
- RA is a systemic disease, and most individuals with the disease experience extra-articular manifestations such as generalized malaise and fatigue.
- Rarely, a patient presents with extra-articular manifestations prior to the onset of arthritis. Some of these manifestations are more common in men (eg, pleural involvement, vasculitis, pericarditis), but the proportion of men and women involved with other manifestations is similar to that of RA overall.
- Rheumatoid nodules
- Rheumatoid nodules occur in approximately 25% of patients with RA, but they occur in less than 10% of patients during the first year of the disease. They are most commonly found on extensor surfaces or sites of frequent mechanical irritation.
- The olecranon process, proximal ulna, back of the heel, occiput, and ischial tuberosities are common periosteal sites for rheumatoid nodule development. Nodules also may form in subcutaneous tissues of the finger, in toe and heel pads, in tendons, and in viscera.
- Rheumatoid factor (RF) is almost invariably present, and if absent, other diagnoses are suggested.
- Frequently, there is a discrepancy between the level of articular inflammation and the progression of nodule formation. Patients with rheumatoid nodulosis have a great number of nodules, usually subcutaneous, and may have little active synovitis. In a similar fashion, patients whose articular inflammation responds well to treatment with methotrexate may have a seemingly paradoxical rapid increase in the number of nodules.
Causes
The cause of rheumatoid arthritis (RA) is still unclear, despite extensive studies of many variables such as endocrinologic, metabolic, nutritional, geographic, occupational, and psychosocial factors (all of which influence the manifestation, but not the frequency, of the disease). Infectious etiologies have been implicated; however, specific inciting agents have not been identified. Data that suggest infectious etiologies include resemblance of RA to caprine arthritis-encephalitis caused by lente viruses, mycoplasmal arthritis in rodents, andErysipelothrix infections in swine. Measles and parvovirus have been cultured from seronegative RA joints. Ongoing studies are investigating these implications.
References
- Williams SB, Brand CA, Hill KD, et al. Feasibility and outcomes of a home-based exercise program on improving balance and gait stability in women with lower-limb osteoarthritis or rheumatoid arthritis: a pilot study. Arch Phys Med Rehabil. Jan 2010;91(1):106-14. [Medline].
- Allaire S, Wolfe F, Niu J, et al. Current risk factors for work disability associated with rheumatoid arthritis: recent data from a US national cohort. Arthritis Rheum. Mar 15 2009;61(3):321-8. [Medline].
- Areskoug-Josefsson K, Oberg U. A literature review of the sexual health of women with rheumatoid arthritis. Musculoskeletal Care. Feb 25 2009;[Medline].
- Ahlmen M, Svensson B, Albertsson K, et al. Influence of gender on assessments of disease activity and function in early rheumatoid arthritis in relation to radiographic joint damage. Ann Rheum Dis. Jan 21 2009;[Medline].
- Jorgensen KT, Pedersen BV, Jacobsen S, et al. National cohort study of reproductive risk factors for rheumatoid arthritis in Denmark - a role for hyperemesis, gestational hypertension, and pre-eclampsia?. Ann Rheum Dis. Mar 15 2009;[Medline].
- Luqmani R, Hennell S, Estrach C, et al. British Society for Rheumatology and British Health Professionals in Rheumatology guideline for the management of rheumatoid arthritis (after the first 2 years). Rheumatology (Oxford). Jan 27 2009;[Medline]. [Full Text].
- Goksel Karatepe A, Gunaydin R, Turkmen G, et al. Effects of home-based exercise program on the functional status and the quality of life in patients with rheumatoid arthritis: 1-year follow-up study. Rheumatol Int. Nov 5 2009;[Medline].
- Kamioka H, Tsutani K, Okuizumi H, et al. Effectiveness of aquatic exercise and balneotherapy: a summary of systematic reviews based on randomized controlled trials of water immersion therapies. J Epidemiol. 2010;20(1):2-12. [Medline]. [Full Text].
- Lemmey AB, Marcora SM, Chester K, et al. Effects of high-intensity resistance training in patients with rheumatoid arthritis: a randomized controlled trial. Arthritis Rheum. Dec 15 2009;61(12):1726-34. [Medline].
- Macedo AM, Oakley SP, Panayi GS, et al. Functional and work outcomes improve in patients with rheumatoid arthritis who receive targeted, comprehensive occupational therapy. Arthritis Rheum. Nov 15 2009;61(11):1522-30. [Medline].
- Goldenberg DL. The interface of pain and mood disturbances in the rheumatic diseases. Semin Arthritis Rheum. Feb 12 2009;[Medline].
- Barry MA, Purser J, Hazleman R, et al. Effect of energy conservation and joint protection education in rheumatoid arthritis. Br J Rheumatol. Dec 1994;33(12):1171-4. [Medline].
- Guccione AA. Physical therapy for musculoskeletal syndromes. Rheum Dis Clin North Am. Aug 1996;22(3):551-62. [Medline].
- Jain R, Lipsky PE. Treatment of rheumatoid arthritis. Med Clin North Am. Jan 1997;81(1):57-84. [Medline].
- Keystone EC, Genovese MC, Klareskog L, Hsia EC, Hall ST, Miranda PC, et al. Golimumab, a human antibody to TNF-{alpha} given by monthly subcutaneous injections, in active rheumatoid arthritis despite methotrexate: The GO-FORWARD Study. Ann Rheum Dis. Dec 11 2008;[Medline]. [Full Text].
- Lipsky PE. Rheumatoid arthritis. In: Isselbacher KJ, Braunwald E, Fauci AS, et al, eds. Harrison's Principles of Internal Medicine. 17th ed. New York, NY: McGraw-Hill; 1994:1648-55.
- Nicholas JJ. Rehabilitation of patients with rheumatic disorders. In: Braddom RL, ed. Physical Medicine and Rehabilitation. Philadelphia, Pa: Saunders; 1996:711-27.
- Nicholas JJ. Physical modalities in rheumatological rehabilitation. Arch Phys Med Rehabil. Sep 1994;75(9):994-1001. [Medline].
- Klippel JH, ed. Primer on the Rheumatic Diseases. 13th ed. New York, NY: Springer; 2008.









No comments:
Post a Comment